

Did you know that there are treatments for COVID that can significantly decrease the chance of serious, deadly outcomes of this disease? Did you know that these are available in the outpatient setting? This all sounds wonderful, and these therapies are indeed excellent tools in our COVID-fighting toolbox. But these treatments have been difficult to come by. Supplies are lacking and accessing them in a timely fashion has been difficult. In response, the Biden/Harris administration is launching a “Test to Treat” initiative to make the process of getting treatment for COVID less cumbersome. But what does “Test to Treat” mean and how does it apply to you and your loved ones? Today we are talking “Test to Treat” – the who, when, where, and what of it all.
First, let’s talk prevention!
An ounce of prevention is worth a pound of cure. This is my entire reason for being as a physician. I want to keep you healthy and prevent disease from happening in the first place! When it comes to contagious disease, vaccines have been one of the greatest preventive measures of all time. Got Polio? No. Measles? Nope! Why? Because vaccines have been highly effective at limiting the spread of contagious illness throughout our communities. If you haven’t gotten your COVID vaccines or booster, please RUN out and do so. And keep sanitizing. Keep your distance from people who are sick. And wear masks in highly crowded areas where you don’t know people’s vaccination status. These measures work!
But for those who are immune suppressed, for whom vaccines may not be as effective, we now have another weapon in our arsenal against COVID-19. Evusheld is a pre-exposure prophylaxis. This means, to help prevent infection, you take it BEFORE you get exposed. Evusheld is a combination of two long-acting monoclonal antibodies. Administration of Evusheld can help prevent COVID infection in immune suppressed persons for up to 6 months! Let’s look at the specifics of this product below.
PS – I created these slides for the American Academy of Family Physicians and they are now property of the AAFP. If making use of these slides, please provide proper attribution to the AAFP. Thanks!!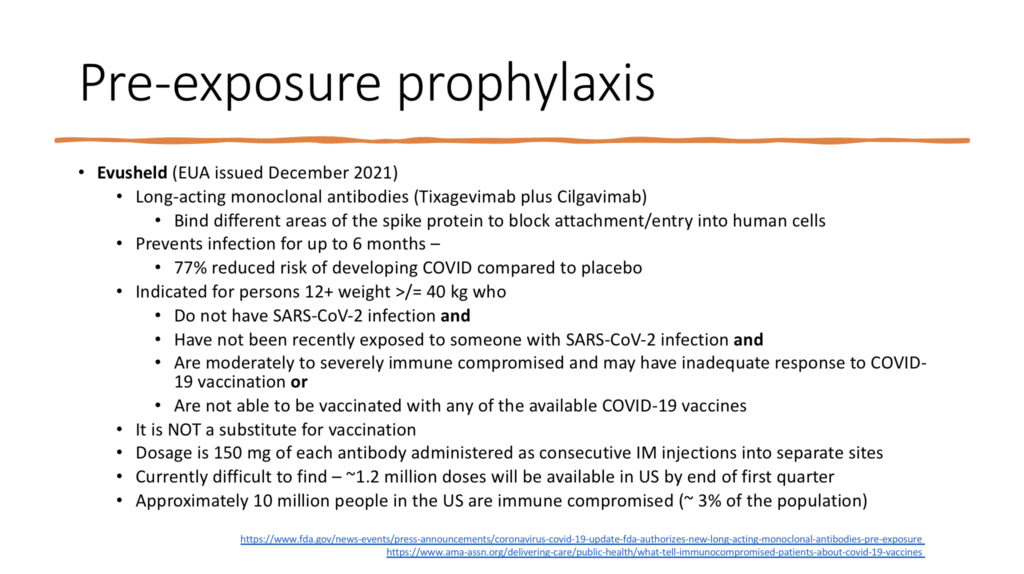
Discussion of pre-exposure prophylaxis with Evusheld. Slide borrowed from the AAFP.
Louder for those in the back – this is NOT a substitute for vaccination. Vaccination is still the best way to prevent infection and serious outcomes of disease. But people with immune suppression, despite being completely vaccinated and boosted, can still get very sick or die from COVID. This is another layer of protection for these high-risk individuals. If you are an immune suppressed person, talk to whomever is providing your immune suppressive care to inquire about how to access this therapy.
But what if prevention fails and you’ve got COVID – now what?
Well, for those of us considered low risk (young, healthy individuals without chronic disease or immune suppression), we do what we’ve always done for viral illness.
- Rest
- Fluids
- Fever reducers, if needed (fever serves a purpose in fighting off infection, however high fever can be harmful. Consider letting it ride its course if low grade. But if 104 or higher, or if a child has a history, for example, of febrile seizures, go ahead and treat to get that fever down).
- Guaifenesin (an expectorant) to help clear mucous
- OTC cough/cold remedies for cough, sore throat, etc.
- Honey to help with cough (NOTE: Never give honey to anyone less than one year of age due to risk of botulism)
- Zinc 75 mg once daily for adults can help decrease the duration of viral illness. More is NOT better (nausea, vomiting, etc.) and do NOT use intranasal zinc (this can cause loss of smell).
But for those who are considered high risk, we now have therapeutics that can shorten the course of illness and decrease the risk of hospitalization and death. Check here to see if you qualify as high risk. The issue with these, and the reason that the “Test to Treat” program offers some hope, is that these treatments have been hard to find. Also, they must be given within a short window of symptom onset to be effective. But those at highest risk may not have easy access to tests. And, in some instances, it can take days to get test results. That short window puts a potential monkey wrench into treatment. Let’s look at the different therapeutic options and who is eligible.
Antiviral therapies
Antiviral medications work in a variety of ways to decrease the virus’ ability to replicate or reproduce itself. We’ll start with Remdesivir. Traditionally this was for use only for hospitalized patients but now we can now give it in the outpatient setting (though it requires a 3-day infusion).
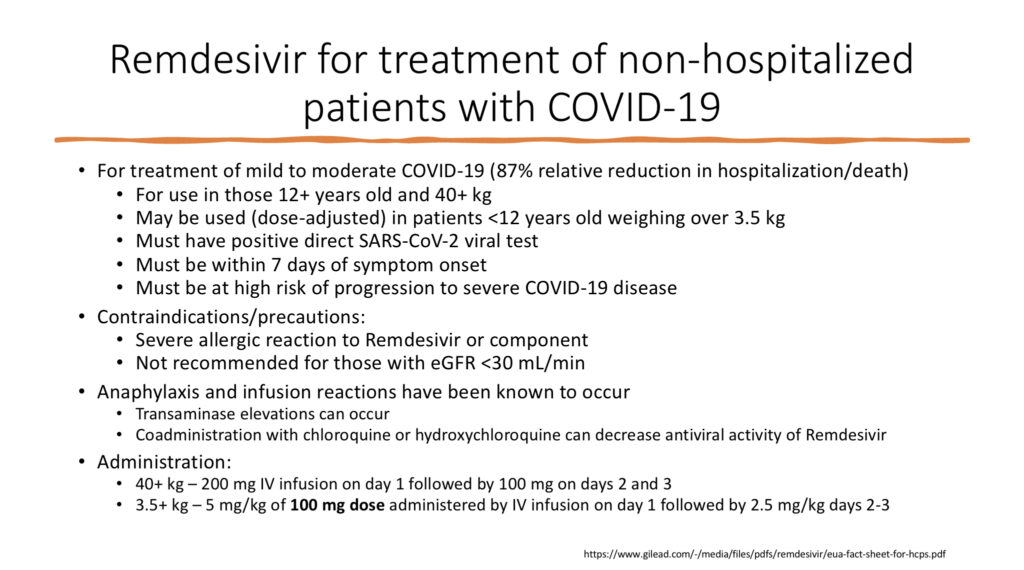
Remdesivir is an antiviral therapy infusion now available for outpatient treatment of COVID illness in high-risk individuals. Slide borrowed from the AAFP.
Quick translation for those who don’t speak doctor, “transaminases” are liver function tests and “eGFR” is a marker of kidney health. And for upcoming slides, “hepatic” refers to the liver and “renal” refers to the kidneys. And now to our oral antiviral options. These, particularly Paxlovid, hold the most promise as the quickest/easiest option to treat. However, both options (Paxlovid and Molnupiravir) come with some notable cautions…
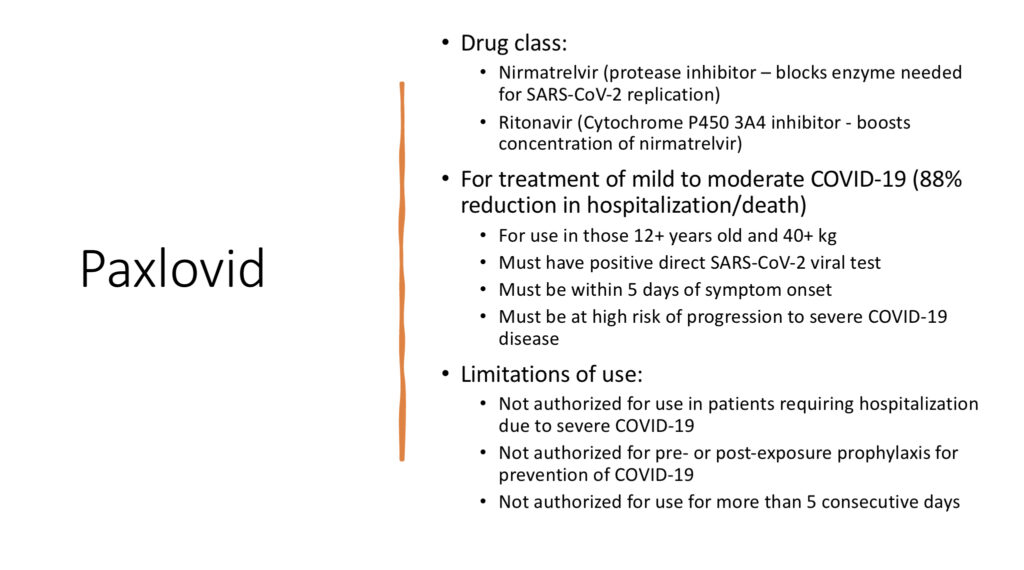
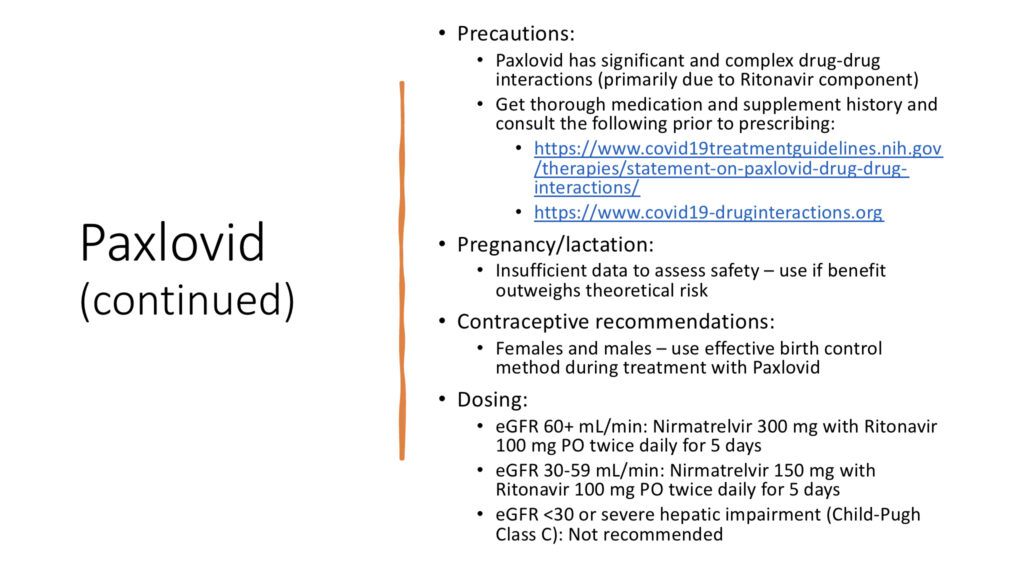
Information on use of Paxlovid oral antiviral therapy to treat COVID-19 in high-risk individuals. Slide borrowed from the AAFP.
The potential for drug interactions is high with Paxlovid. Please go over your medications and supplements in detail with your pharmacist and/or medical provider before taking this medication. Next up, Molnupiravir. This one is probably the least likely candidate for broad use. It has a higher age limitation, significantly lower efficacy rate and concern for potential to alter DNA. But it offers another treatment option if needed.
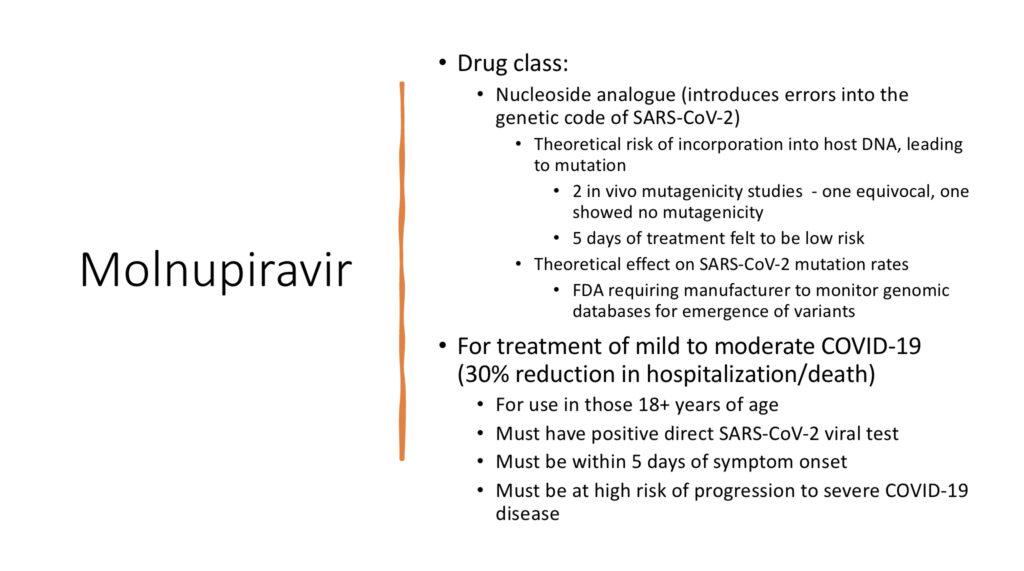
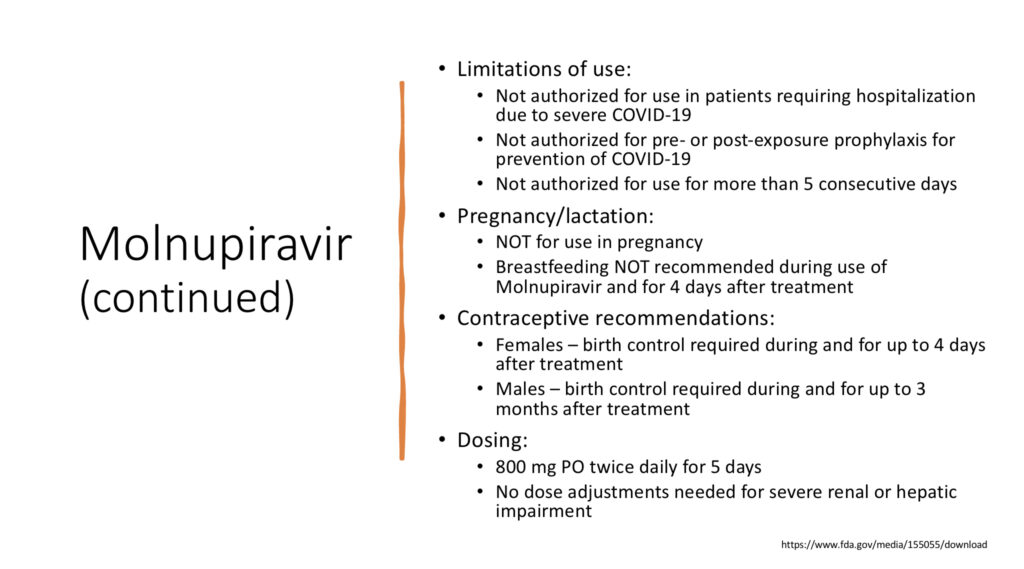
Information on use of Molnupiravir oral antiviral therapy to treat COVID-19 in high-risk individuals. Slide borrowed from the AAFP.
Monoclonal antibody treatments
These work by attaching to the spike protein and blocking entry of the SARS-CoV-2 virus into our cells. We currently have four monoclonal antibody options for treatment of COVID-19 in the outpatient setting. However, the first two (Casirivimab + Imdevimab from Regeneron and Bamlanivimab + Etesivimab from Eli Lilly) are ineffective against the Omicron variant. They are no longer in general use. There may be a place for them in the future, however, depending on effectiveness against future variants. The two shown below (Sotrovimab and Bebtilovimab – who names these things?!?), are our current options available for successful treatment against the Omicron variant. Though, again, this efficacy may change with future variants.
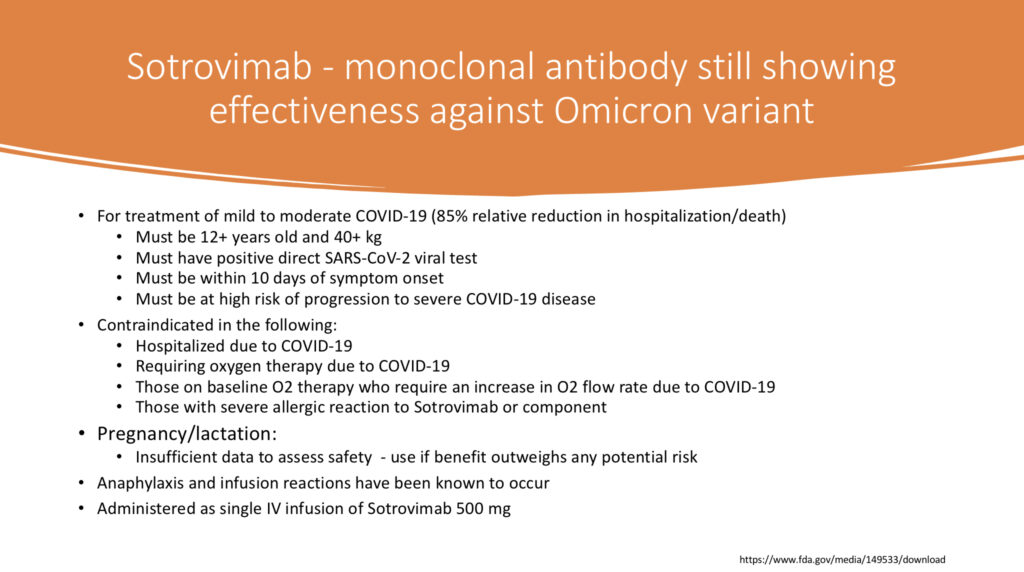
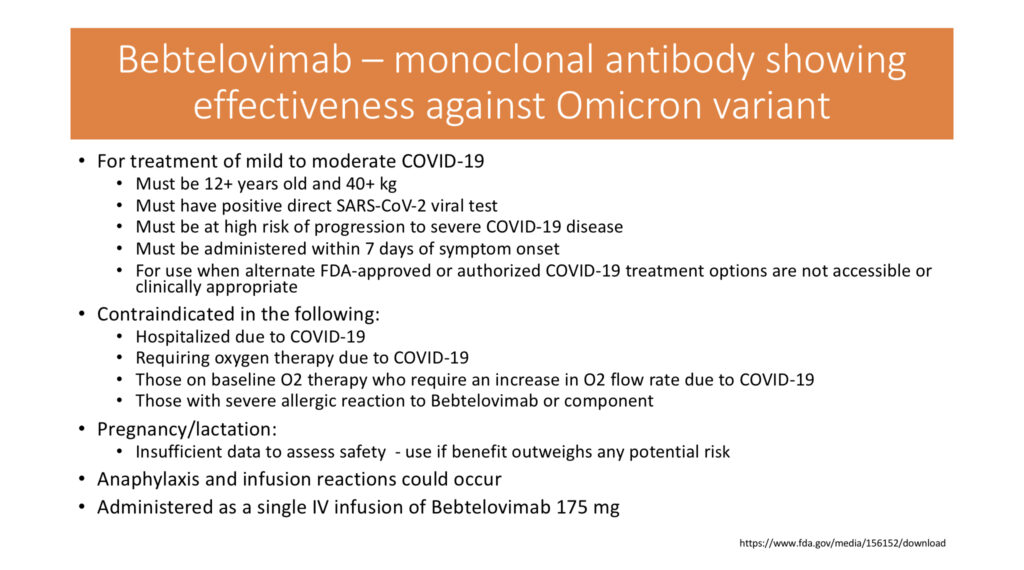
Slides showing indication and information for use of Setrovimab and Bebtilovimab monoclonal antibody therapies for outpatient treatment of COVID-19 in high-risk individuals. Slides borrowed from the AAFP.
Ok, but how much will these therapies cost?
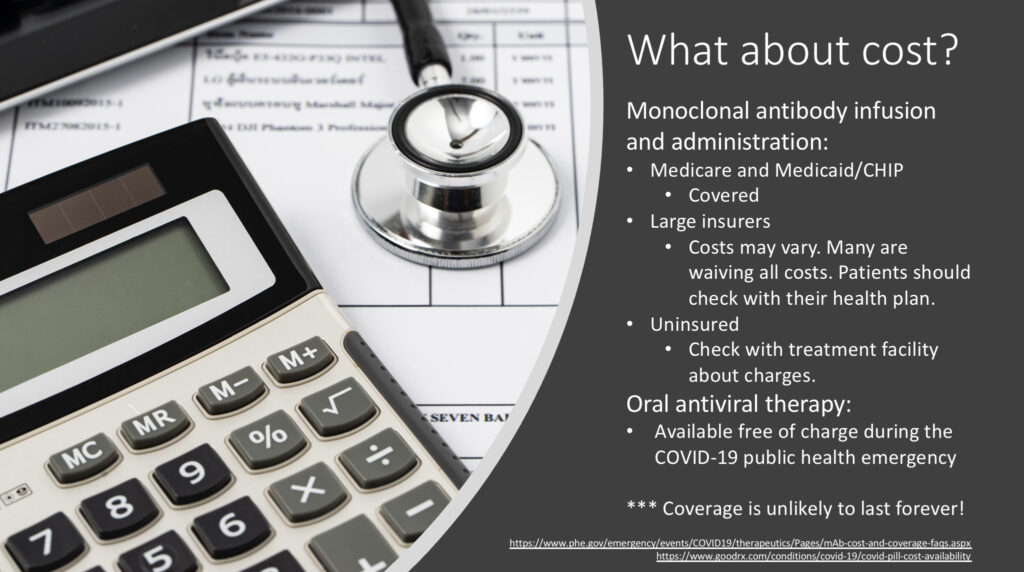
Information about cost to the patient of COVID-19 outpatient therapeutics. Coverage during the public health emergency may not last forever and these therapies are quite expensive. Slide borrowed from the AAFP.
So, what do you do if you are immune suppressed, and you come down with COVID symptoms? The “Test to Treat” program is putting more tests and treatments in the hands of pharmacists and medical providers who provide rapid care. Get yourself to a pharmacy that has a minute-clinic associated with it, or an urgent care, or a local clinic seeing sick patients. Pro tip – you may want to do some calling around and identify these places in your area BEFORE you need them. Test and start treatment, if appropriate.
If you are a medical provider in search of therapies to help your patients, check here for a super handy therapeutics locator!
And remember… YOUR vaccination status impacts all of those around you. To help keep our high-risk loved ones safe, every single one of us needs to vaccinate to create a bubble of protection around those at-risk individuals.
As always, thanks for reading. Please submit any questions or comments and tune in for the next installment by subscribing to my blog (you can find the “subscribe” button on the home page). Until next time…