

All 50 states are reporting cases of the novel Coronavirus. It’s a COVID-19 world now. Is this our new normal? More people are getting tested (though still not enough). The numbers of cases of COVID-19 are surging, and so are deaths from this frightening illness. Every day we read some new headline about risk factors, possible treatments, vaccines, and more. Information is sometimes contradictory and many find it difficult to keep up. We are hearing of scams and shams, playing on the fears of a trusting public. But we are also seeing the best of humanity – people giving generously of their time and resources to help others. It is growing ever more apparent that life will not be getting back to our pre-pandemic routine any time soon.
Information about the Coronavirus Pandemic continues to shift like sand in the tide. As soon as we think we have a footing, the sands move beneath our feet and we are left off balance again. This week’s blogpost will attempt to catch you up on all that has been going on with COVID-19, so that hopefully you will feel a little less off kilter. Admittedly, this is a lofty goal. So, find a comfy chair and settle in. We are going to be here a while.
Let’s begin with a favorite topic…
Here’s what we know –
Most of us are pretty comfortable by now with the basic information about SARS-CoV-2, the virus that causes the COVID-19 illness. But let’s review a few important points.
1. How the virus is spread – SARS-CoV-2 is a virus that is spread by respiratory droplets (coughing, sneezing, etc.) but is also shed in the stool. Covering coughs and proper hand washing or hand sanitizing are HUGELY important to limiting spread.
2. How long the virus lasts on surfaces and in the air – Studies suggest it can survive for up to 72 hours on hard surfaces (like stainless steel or plastic) and up to 24 hours on more porous surfaces (like cardboard). It also appears that the virus can linger in the air (remain aerosolized) for up to three hours. This increases the worry for easy spread and is yet another reason why STRICT ADHERENCE TO SOCIAL DISTANCING recommendations is vital.
3. Who is affected – Initially, it seemed that young people were not as affected by this virus and that the highest risk of death was for those over age 65. Well, this is partly true. However, the most recent analysis of US patients with COVID-19 suggests that younger patients are not without risk. 20% of hospitalizations for COVID-19 occurred in people 20-44 years old and 20% of deaths occurred in those between 20-64 years old. This is NOT just a disease of the elderly.
4. How bad it really gets – It is not “just a bad flu”. It is MUCH MORE CONTAGIOUS and MUCH MORE DEADLY than the flu. Plus, we have no immune memory of this virus. It is a completely new pathogen. We have no built up defenses to fight it off.
5. When we are most contagious – We are most contagious (have the greatest amount of viral shedding) early on in the course of the illness. We can spread the virus to others before we even begin having symptoms. Please. Stay away!
Here’s what we don’t know –
There is still so much that we don’t know about this virus. Here are just a few important questions that we still have to sort out.
1. Are there multiple strains of the SARS-CoV-2 like there are for the flu?
2. Will we develop lifelong immunity to the virus once infected? Antibody testing (see below) will help us figure this out.
3. Why don’t young children seem to be as at risk for complications from COVID-19 as older people?
4. What type of pneumonia do people die from – Is the pneumonia that people die from during a COVID-19 infection a viral pneumonia caused by the SARS-CoV-2 virus or is it a secondary bacterial pneumonia that sets in on top of the already compromised lung tissue? We think it is more of a viral pneumonia but you will hear about people being treated with antibiotics (which shouldn’t help viruses). Basically, we are throwing everything at our severely ill patients, including the kitchen sink. We are trying anything we think might possibly help. Do antibiotics really, paradoxically, work against COVID-19? Time and research will tell.
Here’s what I’m torn on –
1. Really, it’s only one thing… ordering takeout.

From Pixabay
I would love to not have to cook every night and I would love to bolster the economy by supporting our local restaurants. And, yes, I know that the CDC says that infection is not transmitted in food. It is the containers that the food is placed in and subsequently handled by food workers that could be a potential issue. One easily remedied by cleaning off the containers before opening and washing your hands before eating. However, do I trust that every food worker is following the letter of the law with respect to wearing gloves, not touching their faces, and covering their coughs of sneezes as they prepare my food? I have some doubt. So, I’m sorry, but I can’t answer this one for you. This will have to be an individual decision.
Here’s what keeps me up at night –
1. Our medical work force – I woke early this morning with the thought that every physician and nurse may quickly have to step out of their medical comfort zone. When our hospitalists and intensivists fall ill or die from this virus due to lack of adequate PPE (notice, I said when… not if), those of us who haven’t done hospital care in years will be asked to step in. We may have to “jump up a level”. Outpatient clinicians may be asked to man the routine hospital cases. Urgent care docs may be asked to run the ERs. ER docs might have to move up to intensive care. Your psychiatrist, rheumatologist, or dermatologist may be manning the few outpatient primary care cases remaining. Retired physicians and nurses may be asked to come out of retirement. But when you are in crisis mode, what other choice do you have?
2. Those at home in unsafe situations – While many of us may find joy in spending extra hours with our loved ones, this will not be the case for all. Stressful situations and financial strain often worsen the tensions in relationships that already existed. And for some, this is a dangerous scenario. There WILL BE an increase in domestic violence and abuse of all kinds. We need to be watching our family and friends and making sure they are ok. We need to shore up our women and children’s shelters so that they can continue to offer lifesaving services to the community.
What do I make of all the claims I’m hearing on the news and social media?
I think we all recognize that there is both good information and bad, accurate information and inaccurate, to be found in the news and on social media. We certainly can’t believe everything we read on Facebook and Twitter. And even our government officials get it wrong sometimes. So, let’s look at some of these claims and play a game of true or false. Hint: They are all false!
1. The Coronavirus was created in a lab in China – FALSE
a. Researchers have sequenced the genome of the novel Coronavirus and noted it to be most genetically similar to other coronavirus strains found in bats. There is NO evidence to suggest it is man-made. Would China really infect and kill their own people, plunging their economy into a depression, in order to release this virus to other parts of the world? That just doesn’t make sense.
2. If you can hold your breath for 10 seconds, you don’t have Coronavirus – FALSE
a. The suggestion is that COVID-19 causes lung fibrosis (a scarring condition) that decreases the ability to hold a deep breath. Perhaps, if you had serious lung disease from COVID-19 (you’d likely already know you were infected because you’d be in the ICU), you might not be able to hold a breath for 10 seconds. But this does nothing to predict whether you have early illness, which often causes only very mild respiratory symptoms. This is utterly untrue and has the potential to provide people false reassurance.
3. If you gargle with hot saltwater you can prevent Coronavirus – FALSE

Photo of a fotofolio.com postcard. Untitled, 1929. Photographer Unidentified. Copyright FPG International.
a. This claim even circulated in the early 1900s, before a flu vaccine was available – it was wrong then and it is wrong now. Saltwater, warm or cold, can decrease inflammation in the throat and has been a common remedy to ease sore throats for decades. But it does nothing to prevent the SARS-CoV-2 virus from taking hold of receptors on your respiratory tissues and making its invasion. Sorry. I wish it was that easy.
4. Drinking water every 15 minutes will protect you from the Coronavirus – FALSE
a. Nope. And over-consumption of water can actually dilute out important electrolytes in the body, causing heart arrhythmias, weakness, and confusion. This can rarely be deadly. If you have a fever or are coughing you may need to increase your water intake so that you don’t get dehydrated (since we lose fluids from coughing and sweating). But increasing water intake will not prevent you from getting the virus. Generally speaking, your average person needs no more than 8 glasses of water daily to maintain hydration.
5. Using hand or hair dryers will kill the Coronavirus – FALSE
a. The only thing that we know kills the Coronavirus on our bodies is proper hand washing or sanitizing with good old soap and water or alcohol-based hand sanitizers. Blowing hot air into your nasal passages, as some posts suggest we do, would only dry out your nasal passages and put you at risk of burns. Just say no!
6. A national lockdown is coming and troops are being placed to prevent looting and rioting – FALSE
a. There is no evidence to suggest that the government is preparing for a national lockdown.
b. The military and National Guard have been dispatched to some hard hit areas of the country but this was not on direction of the Department of Homeland Security or FEMA. The Stafford Act, to which these false messages refer, is being misinterpreted. It is a federal disaster relief law that activates FEMA to send aid to state and local governments.
7. I’m not contagious unless I’m sick – FALSE
a. Viruses are universally contagious for some number of days (the number depends on the virus) BEFORE people develop symptoms. SARS-CoV-2 is no different. Don’t wait for symptoms to appear to practice social distancing. If you do, it will be too late.
8. I can go back to work after 24 hours without a fever – FALSE
a. Current guidelines suggest, for people with suspected COVID-19 who are not tested (which, let’s admit it, is most of us), that you can return to work after you satisfy three criteria:
• You have had no fever for 72 hours (without the use of fever reducing medications)
• Symptoms (such as cough, etc.) have resolved
• It has been at least 7 days from the onset of symptoms
9. If you have symptoms of Coronavirus, taking NSAIDs (like Naproxen or Ibuprofen) can make it worse – FALSE (for now)
a. People are so desperate to do something that they are throwing out any ideas that seem to have even minor validity. The problem is that most of these claims have not been studied enough for use to know if they are truly accurate or not. And making generalized, sweeping, statements can put people at risk.
b. There is currently no recommendation to take people who are on daily NSAID medications off of those medications.
c. We always use use cautions with these medications because they have the potential to induce stomach ulcers, increase bleeding risk, increase risk of cardiovascular disease, and cause kidney damage if used in high doses for prolonged periods. And severely ill, hospitalized patients (like those with COVID-19) are already at higher risk of these events occurring.
d. Acetaminophen (called Tylenol in the US and Paracetamol in other countries) is safe for use in reducing fevers as long as the package instructions are followed. Use in excess of these recommendations can cause liver toxicity.
e. Because NSAIDs and Acetaminophen work differently, they are generally safe to use together or in an alternating fashion to help control fever, if Acetaminophen alone is not doing the full job.
f. However, you’ll need to stay tuned. Claims such as this are under further investigation, so recommendations are bound to change as we have more information.
10. If you are on blood pressure medications that are ACE-inhibitors or Angiotensin Receptor Blockers (ARBs), you should stop them as these can make the illness worse – FALSE (for now)
a. Again, we are looking for anything to help guide our actions in treating people with COVID-19. But throwing out all these ideas, without adequate study, is unsafe and confusing.
b. We know that the virus binds to the epithelial cells of the lungs and other tissues through ACE2 receptors. Some people are, therefore, questioning the link between a diagnosis of Hypertension and an increased risk of severe COVID-19 symptoms. Could ACE-Is and ARBs, which are commonly used to treat high blood pressure, be to blame?
c. In animal studies – but not human studies – these medicines have been shown to up-regulate ACE2 receptors in the heart. However, these studies were not done in the setting of SARS-CoV-2 infection. Meanwhile, other studies have shown benefit of using these medications to help treat patients with other types of viral pneumonia. I know. Totally confusing.
d. We should NOT be making medication changes based on hypothesis. We need to wait until the evidence is in to make more generalized guideline recommendations.
e. Do NOT stop your blood pressure medications. This could be disastrous!
If all of that is false, what’s true?
1. What’s true is that anyone can catch SARS-CoV-2 and anyone can transmit it to someone else. You can either be part of the solution or part of the problem. Please choose the solution (see #2)!
2. Staying at least 6 feet away from other people, avoiding touching your face, sanitizing surfaces, and proper hand washing are the most important things we can do to protect ourselves and others.
3. This pandemic is going to affect us all – but the way in which it affects us will be different from one person to the next. Our reality is not necessarily another’s. We need to work hard to understand where others are coming from and to give each other some grace during this stressful period.
What can I do to help?
We’ll break this up into two sections – things that are pleasant enough to think about and things that are not pleasant to think about but that are extremely important. Here we go….
The lighter side
From Wikimedia Commons
1. Bring back the victory garden – The victory garden was a wartime effort to grow your own food, so that canned foods and other store-bought items could be sent to the troops. It was one of many conservation efforts put forth during the 1st and 2nd World Wars. Well, I would argue that we are in a war with SARS-CoV-2. With the run on grocery items, and spring now here, it’s the perfect time to break out your green thumb and start growing some of your own food. It gets us outside (which is good for the body and soul), it helps keep us out of populated places like grocery stores, and it is healthier for us to boot!
2. Conserve a square – I don’t know about you but I am a copious toilet paper user. Well, that ship has sailed. How many squares does a person really need? What minimum number of squares will get the job done? We should all think about this the next time we are in the bathroom. If we don’t, we may end up TP poor. Brother… can you spare a square?
3. Donate your PPE – If you work in the construction business, or other industry that uses masks, PLEASE donate your N95 or surgical masks to your local hospital. They need them urgently. If you have gloves or face shields or any other PPE that our health care providers desperately need, please donate them NOW. You could be saving a life.
The darker side
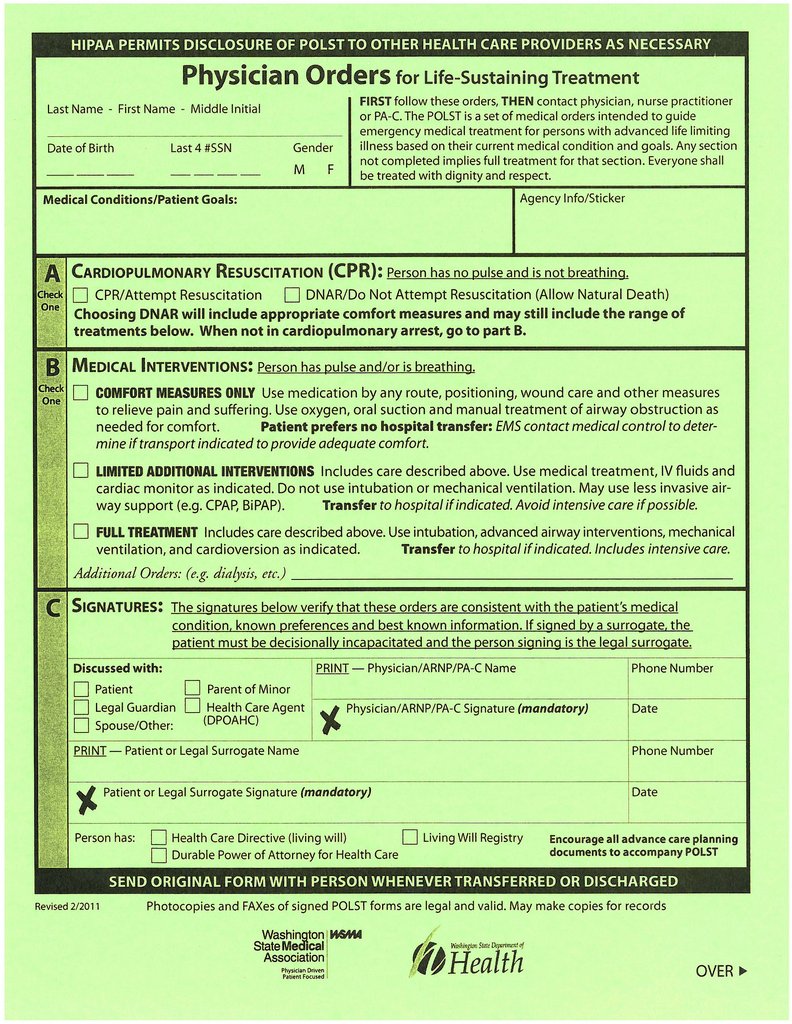
From the Washington State Medical Association
4. Think about your end of life wishes – If you are elderly or someone with baseline severe health issues, think now about how much intervention you want if you get COVID-19. I know this is not a fun topic to discuss but thinking about the end of our days, and what our wishes are for care during that time, has never been more important. Many people with severe illness end up in isolation in the ICU. They are not allowed to see their families for fear of spreading the illness to others. They are dying alone. And they are using ventilators that could be used elsewhere. Doctors and nurses don’t want to have to make tough decisions about who gets a ventilator and who doesn’t. YOU can help make that decision for them.
In Washington state (and likely in other states as well), we have something called the POLST form to help us lay out our wishes. This stands for Physician Order for Life Sustaining Treatment. It is meant to be used by the first responders who come to your house in a medical emergency. There are also Living Wills and you can designate a Power of Attorney (someone to speak for you if you can’t make your own medical decisions) but these have to be drawn up with a lawyer and so are a bit more cumbersome to complete.
The POLST form allows you to indicate if you want to be resuscitated or not in the event that your heart stops beating or you stop breathing. It also allows you to indicate the level of care that you wish (or don’t) were you to end up severely ill enough to qualify for hospital care. Do you just want to be made comfortable and allowed to pass at home? Do you want some intervention if you can return to your previous state of health but don’t want things like IV nutrition or to be put on a ventilator? Or do you want everything done, no matter what? These are the wishes you can lay out on the POLST form.
Traditionally, this is signed by your medical provider and then placed at your bedside or on (or in) the refrigerator. I usually have people put it in a ziploc bag in the freezer. These are places that EMS knows to look if they get called to your house. You can download this form here.
5. Draw up a will – If you are parents with children that would still need caring for in the event of your demise, please think now about who you would have care for your children. Ideally, this is something you’ve already laid out legally. But, if not, now’s the time to write out your wishes. Here’s a site outlining how to make a will without using a lawyer.
Please, Doc. Give me some good news!
There are actually lots of bright spots to be found, if we are willing to look!
1. The constant distraction and harried nature of our lives is changing. We are being forced to slow down and that may turn out to be just what we needed.
2. Medical care is going virtual and, for some, that is a welcome relief.

From Pixabay
There are current restrictions, for the safety of our patients, on who we can see in person in the office. But it turns out that many visits don’t actually require the laying on of hands and can be done via phone or virtual technology. Our home bound patients, who have always had trouble getting into the office, can now get care with their PCP more easily and conveniently. And insurances are now allowing billing for this type of care. Hopefully, going forward, this will facilitate improved access to care for those who are housebound or who live in remote areas without easy access to local medical care.
3. TP supplies are slowly improving – though the word on the street (and by “the street”, I mean my patients) is that chicken is the new toilet paper. What the cluck?
4. Some treatments are showing promise. While it was premature of the president to tell people that they could ask their doctor for Hydroxychloroquine to treat COVID-19, this medication and others are currently being tested and showing some promise of success. Right now they are only being used in the sickest of the sick and are not for prescription to the general public… but that may change based on further research.
• Hydroxychloroquine and Chloroquine – these are antimalarial drugs and are commonly used to treat patients with inflammatory conditions like Lupus. They are felt to have benefit in slowing viral entry into cells and decreasing the viral-mediated inflammatory storm that can lead to organ failure and death. These are already proven generally safe in humans, though have potential to cause QT prolongation (an electrical issue in the heart that can increase the risk of cardiac arrhythmias). Chloroquine has greater potential for toxicity than does Hydroxychloroquine.
• Remdesivir –still in trial with Gilead Sciences laboratories, this RNA virus therapy was originally developed for treatment of Ebola. It is felt to work by blocking RNA replication. It has shown some benefit in treating other Coronavirus illnesses like SARS and MERS and studies looking at benefit against COVID-19 are beginning with several university hospitals around the country.
• Azithromycin – based on a very small French study (20 people treated). Addition of Azithromycin, an antibiotic commonly used to treat bacterial respiratory infections, to Hydroxychloroquine decreased detection of virus in nasopharyngeal samples better than hydroxychloroquine alone. However, this did not evaluate improvement in outcomes, only decrease in detectable viral load.
5. A vaccine is on the horizon.

From Pixabay
Countries around the world are in a race to develop the first vaccine against SARS-CoV-2 and some have even moved into human trials. Because of the prior work on vaccines for SARS and MERS (two other deadly Coronaviruses) we are making more rapid advancements towards a vaccine than would otherwise be possible.
• In Seattle, a human trial is underway testing 45 patients, 15 each at different dose levels. It will evaluate both safety and tolerability, as well as immunogenicity (the ability to induce an antibody/immune response to the virus).
6. We are on the verge of having a SARS-CoV-2 antibody test.
• This will tell us if someone has already been exposed and developed immunity to the virus. Antibody tests are blood tests. They will be relatively easy to acquire and will help us get a better sense of the baseline level of illness in the community.
• This would help scientists model the course of the disease and aid decisions about whether lockdowns or other austere measures are necessary.
• It could tell us if children are not getting sick because they are not getting infected or if symptoms are so mild so as to escape attention. It could help us determine when or if to re-open schools.
• It will also help us to answer questions about how long immunity lasts as we will be able to follow antibody levels over time.
7. More and more people are getting outside for walks, bike rides, etc. to help keep from feeling too penned up. Maybe we’ll turn into a nation of outdoor enthusiasts. Fingers crossed!
8. Pollution is improving, with decreased factory production and a decreased number of cars on the road. At least, for now.
9. Our sense of community is growing by the day. Following several years of divisiveness, this may help bring our country back together.
10. Faith in the medical and scientific communities is being renewed. Science, medicine, and public health are what will save us.
11. Innovation is at an all-time high! This is true of other crisis periods in history, as well. Times of national emergency spark creativity and incite us to make things faster, simpler, better.
12. And finally, here’s my pie in the sky wish. Hopefully, those who have doubts about the value of vaccines will change their tune as they see what can happen when we don’t have vaccines or if we allow immunization rates to fall.
Be safe. Be well. Take care of each other! Until next time…
The Baby Bear of COVID-19 articles. Not too technical, not too alarmist, not too optimistic, not overwhelming, just right.
The points made about takeout are spot on, and things I hadn’t considered before.
This is just the best compliment! Thank you so much, Amber!
Gretchen, thank you and congratulations for an outstanding clear scientific piece of writing that is truly a service to the public. Hats off to doctors like you.
Thank you so much! Take care of yourself and thank you for all that YOU do!
Thank you so much for this, Gretchen. I trust you implicitly so I truly appreciate your blog.
Thank you so much Carrie! Be well and stay safe!